To determine the prevalence of cerebrospinal fluid (CSF) markers associated with inflammation
(i.e., elevated white blood cell count, protein concentration, and CSF-specific oligoclonal
bands) in patients with early active autoimmune encephalitis (AE).
|
Cortical Encephalitis With Overlapping anti-N-methyl-D-aspartate Receptor and Anti-Myelin Oligodendrocyte Glycoprotein Antibodies: Report of Two Cases…
|
Abstract Objectives Seizures are a prominent feature of anti‐N‐methyl‐D‐aspartate receptor (anti‐NMDAR) encephalitis. Nearly half of brain magnetic resonance image (MRI) results are abnormal. The a…
|

You don’t always know where the road you are traveling in life is taking you, but once you get to a certain point in your journey, you can always look back. Sometimes signs you missed were there but written in a cryptic way. It is only after that second look, in retrospect, that we can understand what they were trying to tell us. This is the story of my MOG journey. I feel it is important to tell, because unlike many who suddenly had a changed life, mine changed slowly and the signs were there all along. I am not sure exactly when this started, but my first memory of something being off was when I became extremely tired. Not the normal kind of tired, but the kind that scares you, like you will just stop breathing if you don’t try. I also had pain around my eyes. My doctor did some tests, with no results. After months of pressing the doctor, I was finally told that I had “Chronic Fatigue”. I spent the next two years searching for answers. I prayed a lot. One day, while in our kitchen, I asked my husband if the lights seemed dim. He did not think so. I called my doctor, who by now was frustrated and referred me to a psychiatrist thinking I was depressed. Willing to try anything, I met with the psychiatrist who determined I was not depressed. If anything, I was a little “spun up” that I possibly had a chronic illness and my doctor was not taking me seriously. He recommended getting a new doctor. A few years later, I had one more incident of dimming vision, which went away like the first one. Over time, the tiredness faded. Then in April of 2014, after another cold, I started having eye pain, especially when rolling them around. My doctor gave me antibiotics, but a few days later, it was still so painful and my vision in both eyes started to dim. This time it was it was much worse, darkening by the hour. Panicked, I ran to the eye doctor who saw me immediately and told me I was having a bout of Optic Neuritis (ON). He sent me to Shalom Kelman, an Optic Neurologist, who quickly administered Solumedrol, and I was better. Unfortunately, this did not last. Two days after stopping the medicine, I was blind again and treated. Again and again it happened, ending with a week in the hospital. Luckily, Dr. Kelman referred me to Dr. Michael Levy at Johns Hopkins. He is the world authority on what I learned could be Neuromyelitis Optica (NMO). Dr. Levy took my case and by August, he put it to rest with Rituxan. A blood test for NMO was negative. After repeating this more than once, he said that I was in the group of those who they considered as having NMO but tested negative for it. This happens in about 30% of patients. In other words, I was in the Spectrum Disorder of NMO, or NMOSD. It was all very confusing, and I tried to be brave. Despite the Rituxan, I still suffered attacks about once a year, either in one eye or the other, and once with a small lesion on my spinal cord. This caused progressive weakness and uncontrollable spasms in my legs as well as loss of bladder control. All without much damage. Finally, after my last attack, Dr. Levy decided that maybe it was time to check me for the Myelin Oligodendrocyte Glycoprotein (MOG) antibody, and it was in fact positive. After seventeen years in the making, I finally had my “smoking gun,” MOG Antibody Disease (MOGAD). I am lucky as others are left with bigger scars from this disease. I have to deal with the occasional pain in between my shoulders, and while I can see, I have visual issues. Color is dimmer, I need more light, and I can’t pick things out as quickly in a complicated arrangement of objects. Shopping is not what it used to be and looking for things in a messy drawer sometimes frustrates me. I have had my tears, but I had to find the silver lining. Despite this, still every day is a little scary when your body is a loose cannon. People with colds scare me as I try to be careful not to get sick. Medicine choices are few, and Dr. Levy has changed my preventive treatment to Cellcept, hoping for better control over the attacks. Preventive options for MOG are few, so time is of the essence to find a cure. Because of these struggles, my daughter, Kristina Lefelar, and I decided to start the MOG Project. My good friend, Cynthia Albright, also a newly diagnosed MOG patient, as well as my sister, Amy Ednie, happily made the commitment to join us and we formed the group as co-founders. Since then we have taken in new members: Peter and Pamela Fontanez, whose daughter Isabel overcame a horrific experience with her eventual diagnosis of Multiphasic Acute Disseminated Encephalomyelitis (ADEM/MDEM) and recurrent Optic Neuritis (ON), caused by the MOG antibody; Jen Gould whose daughter Sophia was diagnosed with MOG after a scary illness with Autoimmune Encephalitis (AE) and ON; Andrea Mitchell, who has MOG but was misdiagnosed with Chronic Relapsing Inflammatory Optic Neuritis (CRION), then unnecessarily went blind; and our newest member Chelsea Ednie, my niece, who will help SRNA with social media. These members make up the MOG Squad and we are on a mission to support the community of those who have nowhere to go and are frightened at the prospect of having a rare disease with no cure. Our overall mission is to raise awareness, educate and advance research because, as a rare disease, there is a lot of misinformation, lack of education for patients, caregivers and doctors, and not a lot of research addressing MOGAD. We also continue to work through social media to help others find resources and to understand and advocate for their condition. What a way to make lemonade out of lemons! Things are looking up and for once, the road ahead seems hopeful. Julia Lefelar MEET OUR OTHER HOPE AMBASSADORS
|
Asian Journal of Psychiatry Available online 13 June 2020, 102208 CAPGRAS DELUSION IN ANTI-NMDAR ENCEPHALITIS: A CASE OF AUTOIMMUNE PSYCHOSIS Author links open overlay panel Show more First page preview Open this preview in PDF View full text © 2020 Elsevier B.V. All rights reserved.
|
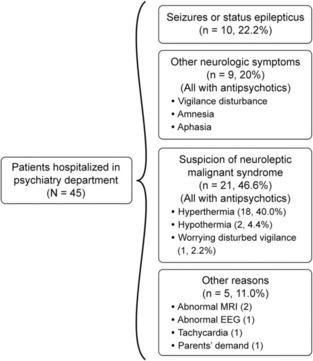
To precisely describe the initial psychiatric presentation of patients with anti-NMDA receptor (NMDAR) antibodies encephalitis (anti-NMDAR encephalitis) to identify potential clues enhancing its early diagnosis.We retrospectively studied the French Reference …
|
|
Brain imaging in catatonia: systematic review and directions for future research – Alexandre Haroche, Jonathan Rogers, Marion Plaze, Raphaël Gaillard, Steve CR Williams, Pierre Thomas, Ali Amad…
|
Abstract Seizures are a well‐recognized and often prominent manifestation of autoimmune encephalitic syndromes. Progress in detection of pathogenic neural autoantibodies has led to increased awaren…
|
NMDA encephalitis is challenging to diagnose in the ED, but a little knowledge can go a long way. This ToxCard provides pearls in the evaluation and management of NMDA encephalitis.
|
The 14 year old girl, was brought to hospital with complaints of one episode of seizure at home followed by another in hospital…
|
Refractory anti-NMDAR encephalitis successfully treated with bortezomib and associated movements disorders controlled with tramadol: a case report with literature review.
|
|