What happens when you have a creative social worker, with an interest in the altered brain, working out of a large city hospital and who …Read More…
|
If there’s one book that I have been eagerly awaiting this year, it is unquestionably The Great Pretender by Susannah Cahalan (available Tuesday, November 5, 2019 from Grand Central Publishin……
|
Learn more about Sage Therapeutics work for the treatment of a range of neurological, neurodegenerative, and neurodevelopment disorders.
|
A severe shortage of immune globulin – a popular medicine used to treat epilepsy, cancer and immune disorders – is forcing doctors nationwide to cancel patients’ lifesaving infusions as hospitals and treatment centers resort to rationing and dose-cutting.
|
Our final national risk management seminar for the year was held in Chicago this past weekend, and two poster contest prizes were determined – best poster of the seminar and the grand prize for the cumulative best poster votes from all four seminars.
|
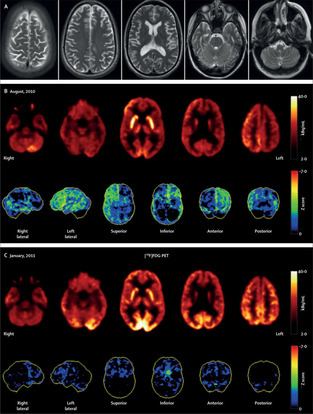
Introduction When cerebral white matter lesions are detected in young patients presenting with neurologic symptoms, the most likely diagnosis is multiple sclerosis (MS). Still, it is crucial to screen for important differential diagnoses which require sophisticated workup and sometimes immediate treatment, such as autoimmune encephalopathies, juvenile stroke, central nervous system (CNS) vasculitis, and, as in this case, Susac syndrome. Knowledge about key clinical and neuro-imaging features is therefore of utmost importance. Here, we report a case of a young woman presenting with encephalopathy, focal neurological deficits, and cerebral white matter lesions and discuss our diagnostic approach. Case A previously healthy 30-year-old woman presented to our emergency department due to a 1-week history of progressive confusion, personality change, vertigo, and stroke-like episodes with temporary aphasia. Clinical examination revealed fine motor impairment of the left hand, bilateral pyramidal signs, and deficits in memory, attention, and executive functions. As the patient was agitated, only a brief magnetic resonance imaging (MRI) protocol (diffusion-weighted, T2 and fluid attenuated inversion recovery [FLAIR] sequences) was performed, revealing multiple supra- and infratentorial punctate diffusion-restricted lesions as well as FLAIR-hyperintense white matter lesions without evidence of restricted diffusion. In addition, the central corpus callosum revealed round (snowball), linear (spoke), and “hanging” (icicles) T2 and FLAIR-hyperintense lesions (Fig. 1, Panel A). Due to these pathognomonic imaging findings, Susac Syndrome, an immune-mediated endotheliopathy of precapillary arterioles of the brain, retina, and inner ear [1], was considered as the most likely differential diagnosis. The patient was admitted to our neurological intensive care unit for observation and further diagnostic workup until potentially life-threatening differential diagnoses had been excluded. Sedation or mechanical ventilation was not necessary. Discussion of Differential Diagnoses Cerebrospinal fluid (CSF) analysis revealed a normal cell count, which made an infectious etiology unlikely. Still, she was treated with intravenous aciclovir (10 mg/kg bodyweight every 8 h) for 24 h until negative results for herpes virus polymerase chain reaction were obtained. CSF protein was mildly elevated (98 mg/dl, normal range < 60 mg/dl), indicating dysfunction of the blood–brain barrier, and intrathecal immunoglobulin synthesis was detected. Screening for antibodies against neuronal surface and intracellular antigens as well as for thyroid antibodies was negative, arguing against the differential diagnosis of autoimmune encephalitis or encephalopathy including steroid-responsive encephalopathy associated with autoimmune thyroiditis. Based on the clinical presentation and neuro-imaging findings (lesions in the central corpus callosum), as well as the pronounced dysfunction of the blood–brain barrier (indicated by the highly elevated CSF-to-serum albumin ratio > 47), the differential diagnosis of MS was unlikely. After proper treatment of the agitated state, an extended MRI protocol with susceptibility-weighted sequences and contrast-enhanced angiography was performed but did not reveal vascular abnormalities or signs of hemosiderin deposition. A thorough screening for other organ manifestations including systemic vasculitis was uneventful. Despite the lack of biopsy results, CNS vasculitis was therefore not considered as plausible differential diagnosis. Uneventful transesophageal echocardiography and laboratory screening for antiphospholipid syndrome and other coagulopathies made juvenile stroke unlikely. The diagnosis of Susac syndrome was finally confirmed by retinal fluorescein angiography (Fig. 1, Panel B), showing multiple branch retinal artery occlusions and arterial wall hyperfluorescence, and by pure-tone audiometry revealing hearing loss for low- and mid-tone frequencies. After high-dose intravenous methylprednisolone therapy (1 g/day for 3 days) and intravenous immunoglobulin administration (2 g/kg bodyweight over 2 days), neuropsychological and motor symptoms markedly improved. Treatment was continued with oral methylprednisolone (1 mg/kg bodyweight with slow tapering), mycophenolate mofetil (2 g/day), and intravenous immunoglobulins (1 g/kg bodyweight every other week). After 3 months (five cycles of intravenous immunoglobulins), the patient had fully recovered except for mild hearing deficits. Neuro-imaging did not reveal new lesions. Therefore, so far, no treatment intensification in terms of adding tacrolimus, cyclophosphamide, or rituximab was necessary. It is important to mention that the patient never suffered from headache and CSF examination revealed intrathecal immunoglobulin synthesis, which is both not typical for Susac syndrome and made a broad laboratory and neuro-imaging workup necessary. Conclusion Susac Syndrome is a rare but probably under-recognized condition typically manifesting with headache, encephalopathy, and focal neurological signs. It occurs primarily in young women (3–4 times more often than in men) at a median age of 30–35 years at onset [2] and affects the microvasculature of the brain, retina, and inner ear. Pathophysiologic mechanisms are incompletely understood; however, histopathologic findings and clinical improvement after initiation of immunosuppressive therapy strongly suggest an immune-mediated mechanism. The full diagnostic triad consists of (1) neurological manifestations and typical MRI findings (brain involvement), (2) branch retinal artery occlusions or arterial wall hyperfluorescence in retinal fluorescein angiography or signs of retinal branch ischemia in fundoscopy or optical coherence tomography (retinal involvement), and (3) new tinnitus, hearing loss or peripheral vertigo (cochlear involvement). Recommended treatment includes corticosteroids, intravenous immunoglobulins, and mycophenolate mofetil [3]. Depending on disease severity, tacrolimus, cyclophosphamide, or rituximab may be added. Treatment for at least 2 years is recommended [3]. Important differential diagnoses include MS, CNS vasculitis, autoimmune encephalopathies, and juvenile stroke.
|
The autoimmune encephalitis (AE) syndromes have been characterised by the detection of autoantibodies in serum and/or cerebrospinal fluid which target the
|
PubMed comprises more than 30 million citations for biomedical literature from MEDLINE, life science journals, and online books. Citations may include links to full-text content from PubMed Central and publisher web sites.
|
Abstract Objective Autoantibody detection is crucial for the early diagnosis of autoimmune encephalitis (AIE) since prompt therapy can determine the disease outcome. Here, we report a single‐center…
|
Antibodies in CSF specific for viral peptides implicate enteroviruses in acute flaccid myelitis.
|
|
PubMed comprises more than 30 million citations for biomedical literature from MEDLINE, life science journals, and online books. Citations may include links to full-text content from PubMed Central and publisher web sites.
|

In the interdisciplinary and translational research group SYNABS, experts from the fields of neurology, physiology, neuroimmunology and neuropathology will investigate the disease mechanisms of autoimmune encephalitis. Their aim is to develop targeted therapeutic approaches for this disease, which is often accompanied by psychological symptoms. Autoimmune encephalitis was first described in medical literature over 10 years ago and, in the meantime, neuroscientists have identified a whole family of these rare diseases, which primarily affect young adults. Triggered by certain tumours or infections or, most commonly, without any identifiable cause, antibodies are produced against neurotransmitter receptors in the central nervous system and these disrupt signal transmission to the neuronal contact points, the synapses. Consequences can include disorientation, psychosis, epileptic attacks or impaired consciousness. To gain a better understanding of the disease mechanisms “The aim of the SYNABS research group is to develop a detailed understanding of the mechanisms of the various forms of autoimmune encephalitis,” explains group spokesman Christian Geis from Jena. The working group led by Josep Dalmau in Barcelona, who is regarded as a pioneer in the field of antibody-mediated encephalitis, is also associated with the study. Specialists from clinical-experimental research and also basic scientists with particular methodological expertise will work on eight sub-projects.
|
This interview will be on “St. Louis on the Air” during the noon hour on Tuesday. This story will be updated after the show.Here are some ways to listen…
|
Background: In recent years, the phenomenon of coexisting systemic autoimmune diseases (ADs) in patients with autoimmune encephalitis (AE) has been increasingly found, while its clinical significance…
|
“The Great Pretender,” the new book by the author of “Brain on Fire,” is another medical detective story, but this time the person at the heart of the mystery is a doctor, not a patient.
|
PubMed comprises more than 30 million citations for biomedical literature from MEDLINE, life science journals, and online books. Citations may include links to full-text content from PubMed Central and publisher web sites.
|
Abstract In clinical practice, involuntary vocalizing behaviors are typically associated with Tourette syndrome and other tic disorders. However, they may also be encountered throughout the entire …
|
There is increasing recognition in the neurological and psychiatric literature of patients with so-called isolated psychotic presentations (ie, with no, or minimal, neurological features) who have tested positive for neuronal autoantibodies (principally N-methyl-D-aspartate receptor antibodies)…
|
The field of paraneoplastic neurological syndromes PNS has grown exponentially with the increased identification of associated antibodies. Testing for these ant…
|
|